SARS-CoV-2 infection of the nervous system: A review of the literature on neurological involvement in novel coronavirus disease-(COVID-19)
DOI:
https://doi.org/10.17305/bjbms.2020.4860Keywords:
Coronavirus disease 2019, COVID-19, coronavirus, severe acute respiratory syndrome coronavirus 2, SARS-CoV-2, pandemic, nervous system, central nervous system, CNS, peripheral nervous system, PNSAbstract
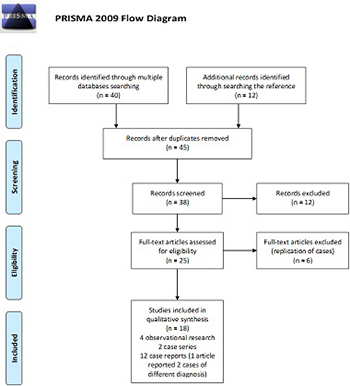
The novel coronavirus disease 2019 (COVID-19) is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which is believed to have emerged from an animal source and has been spreading rapidly among humans. Recent evidence shows that SARS-CoV-2 exhibits neurotropic properties and causes neurological diseases. Here, we review the literature on neurological involvement in SARS-CoV-2 infections and the possible mechanisms of invasion of the nervous system by this virus, to provide a summary and critical analysis of the early reporting of neurological involvement in COVID-19. An exhaustive search of scientific articles on neurological involvement in COVID-19 was performed in the Web of Science, Scopus, Medline/PubMed, and several other databases. Nineteen relevant articles that had been published or were in preprint were carefully selected according to the inclusion and exclusion criteria. Based on our research, we found that patients with COVID-19 can present with neurological symptoms that can be broadly divided into central nervous system involvement, such as headache, dizziness, altered mental state, and disorientation, and peripheral nervous system involvement, such as anosmia and hypogeusia. Most of these patients are in the older age group and exhibit comorbidities, especially hypertension, and severe infection. In extreme presentations of COVID-19, some patients exhibit seizures, stroke, flaccid paraparesis, corticospinal weakness, and even coma. Moreover, the neurological manifestations can occur independently of the respiratory system. In conclusion, SARS-CoV-2 infection can cause multiple neurological syndromes in a more complex presentation. Therefore, this review elucidated the involvement of the nervous system in SARS-CoV-2 infection and will hopefully help improve the management of COVID-19.
Citations
Downloads
Downloads
Additional Files
Published
Issue
Section
Categories
How to Cite
Accepted 2020-05-30
Published 2020-08-03