Percutaneous coronary intervention assisted by invasive mechanical ventilation and intra-aortic balloon pump for acute myocardial infarction with cardiogenic shock: Retrospective cohort study and meta-analyses
DOI:
https://doi.org/10.17305/bjbms.2019.4500Keywords:
Invasive mechanical ventilation, IMV, intra-aortic balloon pump, IABP, percutaneous coronary intervention, PCI, mechanical circulatory support, acute myocardial infarction, cardiogenic shockAbstract
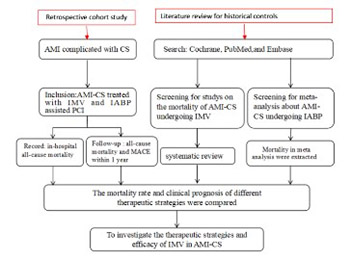
There is little evidence to recommend the optimal invasive mechanical ventilation (IMV) modes and ideal positive end-expiratory pressure stress levels for acute myocardial infarction-cardiogenic shock (AMI-CS) patients. The aim of this study was to compare the mortality outcome in patients with AMI-CS who were treated with percutaneous coronary intervention (PCI) assisted by intra-aortic balloon pump (IABP) + IMV with historical controls. From January 1, 2016 to June 1, 2017, 60 patients were retrospectively enrolled at Tianjin Chest Hospital. Out of these, 88.3% of patients achieved thrombolysis in myocardial infarction (TIMI) flow 3 after PCI. The all-cause mortality rate in-hospital and at 1 year was 25% (95% CI: 0.14–0.36) and 33.9% (0.22–0.46), respectively. A systematic review followed by meta-analysis was performed with four historical studies of patients treated by PCI + IMV with partial IABP, which found an in-hospital mortality rate of 66.0% (95% CI: 0.62–0.71). Recently, a meta-analysis of patients receiving PCI + IABP with partial IMV showed that the 1 year mortality rate was 52.2% (95% CI: 0.47–0.58). In Cox regression analysis of patient data from the current study, lactic acid level ≥4.5 mmol/L, hyperuricemia, and TIMI flow <3 were independent predictors of death at 1 year. All-cause mortality, in-hospital and at 1 year, in patients with AMI-CS treated with PCI + IABP and IMV was lower than in those treated with PCI + partial IABP or IMV. Larger, longer-term direct comparisons are warranted.
Citations
Downloads
Downloads
Additional Files
Published
Issue
Section
Categories
How to Cite
Accepted 2019-11-26
Published 2020-11-02





